The maxillary sinus is a hollow chamber lined by pseudostratified columnar epithelial cells that make up the Schneiderian membrane. In a healthy sinus, mucous production helps clear the sinus of foreign particles and microbes. The base of the maxillary sinus often rests on the bone superior to the roots of the maxillary teeth.
The posterior maxilla consists of bone that is highly trabeculated and often has the lowest density in the mouth. While the mandibular bone can be as dense as oak wood, in comparison, the posterior maxilla can have the density of pine or even balsa wood. To further complicate matters, after the loss of the posterior teeth the maxilla resorbs in a palatal and superior direction, and the maxillary sinus elongates down to reduce the available native bone height.
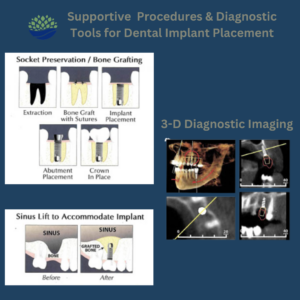
These unique challenges in native bone availability combined with the higher occlusal forces in the posterior jaw lead to the posterior maxilla traditionally experiencing the highest dental implant failure rate. This is especially true when the limits are pushed, i.e. a very short implant is used with a long crown height. However, through innovation in bone augmentation techniques patients can have implant restorations in this region now with equal success rates to all other areas of the mouth. Sinus lift or augmentation surgery can assist implant placement by raising the sinus floor to develop more bone.
Two general techniques for a sinus augmentation exist. The first, called a crestal approach or indirect sinus “tap” involves drilling the planned implant osteotomy short of the sinus floor, then using an osteotome or other instrument to elevate the remaining bone, add additional bone graft in the site, then place the dental implant. This technique is appropriate for sites where 7+ mm of native bone remain before the procedure.
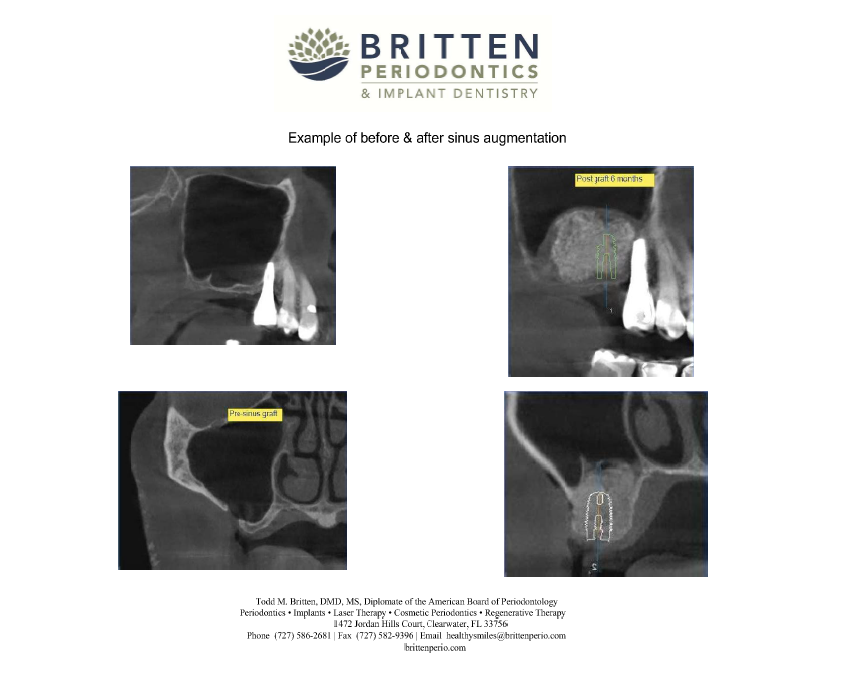
The second technique, called a lateral window or direct sinus graft, involves elevating a periodontal flap and creating an osteotomy window at the lateral aspect of the maxillary sinus in order to elevate the sinus membrane and add bone graft. This may be done as a separate procedure or together with placing the dental implant.
Between 5-8 months is expected for complete healing of the graft. The lateral window sinus graft is appropriate when 6 mm or less of native bone exist as seen on a CT scan. Both sinus augmentation techniques are most often done under conscious sedation in our office.
Since 2015, we have added L-PRF technology to all of our sinus grafts. Leukocyte-Platelet Rich Fibrin is derived from the patient’s own blood. A simplified chairside procedure results in the production of a thin, compressed layer of platelet rich fibrin that is strong, pliable and suitable for suturing. This natural fibrin network is rich in platelets, growth factors and cytokines that are derived from the blood platelets and leukocytes, improving not only bone growth but also natural infection defense. This is typically combined with a 50:50 mixture of bovine (cow) and human donor bone graft material. The results have been excellent! Our lateral window sinus grafts have shown a 98% infection free success rate in that time. Healing is typically easier than expected and many patients even report that their sinuses actually feel better and clearer than before the surgery!
If you or your team have any question about sinus augmentation procedures, please contact us at any time. As always, we are committed to continuing to work with all of you to provide our patients with the highest level of care available.
Click here for a Zimmer Sinus Augmenation Brochure for Patients
 [iphorm id=”3″ name=”Contact form”]
[iphorm id=”3″ name=”Contact form”]