If you have dental implants, you’re expecting them to last a many years, or perhaps a lifetime. In most cases they do, giving patients a fully restored, beautiful, functional smile. Experts estimate between 3-20% of implants fail. This is often due to peri-implantitis – which is a threat to the lifespan of dental implants. Peri-implantitis is gum disease around an implant that is not reversible without intervention by a periodontist or dental implant specialist.
DISEASE AROUND IMPLANTS MIMICS PERIODONTAL DISEASE
There are two categories of complications with implants: Peri-Implant Mucositis and Peri-Implantitis.
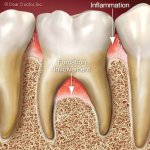
Peri-Implant Mucositis: This condition is similar to gingivitis around a natural tooth and does not include loss of attachment (bone or gum tissue) and is hopefully reversible at this stage. Peri-Implant Mucositis is a reversible inflammatory reaction in the soft tissues surrounding a functioning implant. Treating this condition as soon as possible will prevent peri-implantitis!
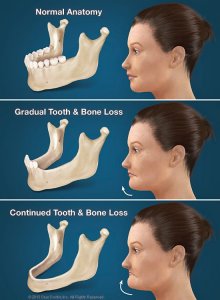
Peri-Implantitis: This is a condition similar to periodontitis with loss of supporting structures (gum and/or bone) around a natural tooth. Peri-Implantitis is a destructive inflammatory reaction affecting the soft (gingiva) and hard (bone).
Signs/Symptoms of moderate-advanced Peri-Implantitis
| SWELLING IN THE GUMS
IMPLANT MOBILITY
BLEEDING GUMS
CHANGE IN GUM COLOR SURROUNDING IMPLANT |
HIGH GUM SENSITIVITY
IMPLANT EXPOSURE (GUM RECESSION PREVENTS ADHERENCE TO THE IMPLANT OR CROWN SURFACE)
MILD TO SEVERE PAIN AROUND IMPLANT SITE
EXCRETION OF PUS FROM THE IMPLANTS SURROUNDING TISSUES |
The good news is that peri-implantitis is treatable, especially if the infection is treated early. In order to help patients catch peri-implantitis, your Clearwater periodontist, Dr. Todd Britten is sharing what peri-implantitis is and how it can be treated with laser surgical therapy, or the LAPIP procedure.
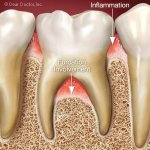
Peri-implantitis is a bacterial infection of the gum and bone around the implant.
LAPIP® is a minimally-invasive method of laser gum disease treatment for implants that helps regenerate healthy tissue instead of destroying it. For most people who have dental implants, LAPIP® is simply the best solution for gum disease around implants, also known as “peri-implantitis”.
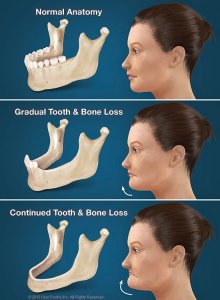
Peri-implantitis is an infection that has much in common with periodontitis, or advanced gum disease. With both diseases, the gums and supporting structures in your mouth are infected and become inflamed. As these diseases progress, pockets of bacteria form below the gum line, creating protected spaces which harbor bacteria and debris, exacerbating the infection. Severe cases of both peri-implantitis and periodontitis lead to bone loss, which can compromise the stability of your teeth or your implant.
If you think you have gum disease, you will need to seek treatment, since both periodontitis and peri-implantitis are progressive diseases which cannot be treated at home. The same daily hygiene used to avoid gum disease can be used to protect against peri-implantitis. You should brush and floss every day, and schedule regular checkups with your dentist, dental implant specialist and periodontist. Finally, certain lifestyle choices, like tobacco use, can increase the risk of gum infections.
Periodontal disease is common, peri-implantitis is less common, occurring in around 1 out of 10 implant recipients. Peri-implantitis is also different from periodontitis because it’s harder to diagnose early. Many patients don’t know they have an infection until serious symptoms develop. More often, peri-implantitis is detected through an x-ray during a regular checkup.
There are several treatment options for peri-implantitis. Surgery or laser procedures are the most common, and of the two, laser treatment is by far the least invasive. LAPIP is similar to LANAP, the procedure used to treat periodontitis. LAPIP, however, is designed to target infection around dental implants.
First, a laser is inserted beneath the gums at the base of the implant, where it targets and destroys bacteria and infected tissue. Ultrasonic tools are then used to remove any remaining bacteria and to make sure the implant is 100% free from dangerous debris. The laser is inserted below the gum line one more time to eliminate any surviving bacteria, and the gums are encouraged to heal around the implant again.
LAPIP treatment offers many important benefits. First, it is less invasive than surgery and does not destroy any healthy gum tissue. The laser is specifically designed to only target infected tissue. This treatment is also quick and effective. Finally, the laser works to stimulate gum and bone growth, allowing your natural bone to increase in both density and mass without a bone graft, protecting the security of your implant for years to come.
Sometimes, the gum tissue surrounding an implant can become thin, and expose the threads of the implant surface below. In this case, Dr. Britten has developed a state-of the-procedure which combines use of the PerioLase laser to destroy bacteria, decontaminate the implant surface and surrounding tissues, and reduce inflammation. Dr. Britten can then perform a procedure to graft tissue around the implant in such a way as to cover the exposed portion of the implant, however, the main objective is to reestablish the protective barrier or layer of the gum around the implant.
If you have implants and think you have peri-implantitis, please contact us immediately. We at Britten Periodontics are committed to providing our patients with the highest level of care available.